Clostridioides Difficile Infection (CDI)
Clostridioides difficile infection (CDI) is defined as:
- 3 or more episodes of loose stool within 24hrs i.e. Bristol stool chart types 5-7 and
- Diarrhoea that is not attributable to any other cause or therapy, including medicines such as laxatives and
- The presence of a positive toxin assay and/or endoscopic evidence of pseudo-membranous colitis.
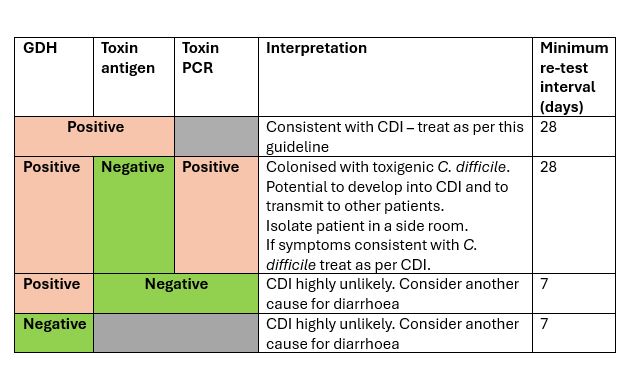
C. difficile stool sample testing has changed and requires interpretation. See additional information section at end of guideline for more details about the test.
Below is a table summarising interpretation of C. difficile lab results:
Always assess the severity of CDI:
Life-threatening CDI includes hypotension non-responsive to fluid filling, partial or complete ileus or toxic megacolon, or CT evidence of severe disease or bowel perforation.
Severe CDI is associated with:
- Acute abdomen: Ileus, peritonitis, perforation
- Temperature over 38.5°C
- White Cell Count (WCC) of 15 x109/L or greater
- Acutely rising serum creatinine (more than 50% increase above baseline)
- Imaging: megacolon, colonic wall thickening, pericolonic fat stranding
Moderate CDI is associated with a raised WCC that is less than 15x109/L. Typically associated with 3–5 stools per day.
Mild CDI is not associated with a raised WCC. Typically associated with less than 3 stools of type 5–7 on the Bristol Stool Chart per day.
Empirical treatment of suspected or confirmed CDI: mild, moderate or severe disease
- Consider IV fluids and electrolyte correction.
- Maintain stool chart.
- For severe disease, refer to Micro/ID and gastroenterology.
- Treat for 10 days
First line: vancomycin 125mg po qds for 10 days
- If the patient fails to respond to vancomycin after 7 days, consult Micro/ID who may advise to switch to fidaxomicin 200mg bd for 10 days.
- Use clinical judgement to determine whether antibiotic treatment for C. difficile is ineffective. It is not usually possible to determine this until day 7 because diarrhoea may take 1 to 2 weeks to resolve.
- For patients with enteral feeding tube or swallowing difficulties order vancomycin liquid or fidaxomicin liquid from pharmacy.
Empirical treatment of suspected or confirmed CDI: life-threatening
Urgent referral to gastroenterology on-call doctor and Micro/ID
- Supportive measures: resuscitate patient with IV fluids and correct electrolytes
- Commence/maintain stool chart
- Abdominal imaging
*When patient is able to tolerate oral medication the metronidazole can be changed to metronidazole 400mg po tds.
- Always discuss treatment of life-threatening cases with Micro/ID as broad-spectrum antibiotics may also be indicated if another condition is being treated.
- If the patient fails to respond to vancomycin and metronidazole after 7 days, consult Micro/ID who may advise to switch to fidaxomicin 200mg bd for 10 days.
- Use clinical judgement to determine whether antibiotic treatment for C. difficile is ineffective. It is not usually possible to determine this until day 7 because diarrhoea may take 1 to 2 weeks to resolve.
- For patients with enteral feeding tube or swallowing difficulties order vancomycin liquid or fidaxomicin liquid from pharmacy.
Relapse
Relapse of CDI symptoms within 12 weeks of initial treatment (with positive CDT stool test): fidaxomicin 200mg po bd for 10 days
For patients with enteral feeding tube or swallowing difficulties order fidaxomicin liquid from pharmacy.
Recurrence
Recurrent episode of CDI after 12 weeks of initial treatment (with positive CDT stool test): Seek ID Micro / Gastroenterology advice.
Treatment options include:
vancomycin 125 mg po qds for 10 days
OR
fidaxomicin 200 mg po bd for 10 days
For patients with enteral feeding tube or swallowing difficulties order vancomycin liquid or fidaxomicin liquid from pharmacy.
2 or more previous confirmed CDI episodes
Recurrent episode of CDI after 12 weeks of initial treatment (with positive CDT stool test): Seek Micro/ID and Gastroenterology advice.
Consider Faecal Matter Transplant (FMT, IPG485) or tapering vancomycin (as below)
Tapering vancomycin course:
- 125mg po qds for 10 days, then,
- 125mg po bd for 7 days, then,
- 125mg po od for 7 days, then,
- 125mg po once every 2 or 3 days for 2 to 8 weeks.
For patients with enteral feeding tube or swallowing difficulties order vancomycin liquid from pharmacy.
Additional information
- GDH tests for the presence of C. difficile but further testing is required to see if the strain can produce toxin as not all strains of C. difficile have the gene that produces toxin.
- The toxin assay tests for current toxin production i.e. toxin antigen.
- The toxin PCR tests for a strain that has the ability to produce toxin. This test is performed when the GDH test is detected and the toxin antigen test is negative.
- Bacteria that cannot produce toxin (toxin antigen and toxin PCR negative for toxin) are not pathogenic.
- The toxin gene may be present but toxigenic strains of C. difficile can live harmlessly in the colon without producing toxin. These strains however can transmit to others or switch to producing toxin.