Prevention of secondary meningococcal disease
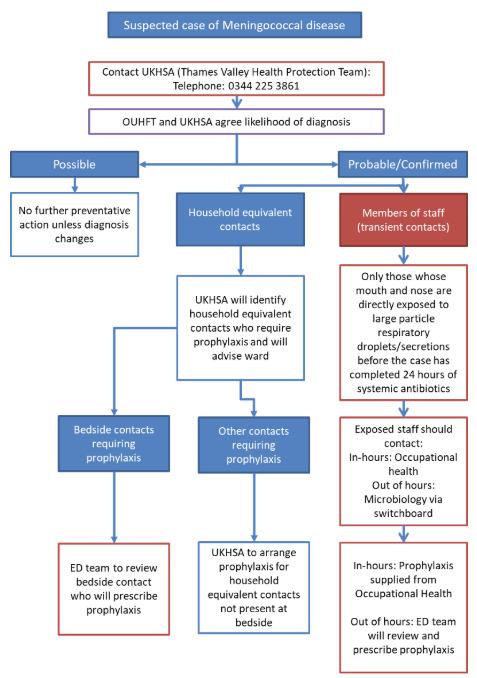
Flow chart of actions for chemoprophylaxis for contacts of Meningococcal case
All suspected cases of invasive meningococcal disease are statutorily notifiable by registered medical practitioners to the responsible health protection team
Possible case:
- Clinical diagnosis of meningitis, septicaemia or other invasive disease where another diagnosis is more likely than invasive meningococcal disease
Probable case:
- Clinical diagnosis where meningococcal infection considered most likely, OR;
- Where there is doubt about the causative agent but the patient has evidence of a serious bacterial infection,OR;
- Where Neisseria meningitidis could be responsible and there is no alternative diagnosis at that time OR;
- Cases of meningitis or septicaemia with clinical and lab evidence of bacterial infection but causative pathogen is not known
Confirmed case:
Clinical diagnosis of meningitis, septicaemia or other invasive infection; AND AT LEAST ONE OF:
- N meningitides isolated (from a normally sterile site);
- Gram-negative diplococci (from a normally sterile site);
- Meningococcal DNA from PCR (from a normally sterile site);
- Meningococcal antigen in blood, CSF or urine;
- Although not meeting the definition of a confirmed case, meningococcal infection of the conjunctiva is considered an indication for public health action (i.e. treatment for the case and antibiotic prophylaxis for close contacts, but not vaccination) because of the high immediate risk of invasive disease.
Key message
Chemoprophylaxis is only recommended for staff whose mouth or nose is directly exposed to large particle droplets/secretions from the respiratory tract of a probable or confirmed case of meningococcal disease during acute illness before the case has completed 24 hours of systemic antibiotics. In practice this means being coughed on directly by the patient or being involved in intubation. If appropriate PPE was worn chemoprophylaxis is not required.[1]
Chemoprophylaxis
1. Members of Staff
1.1. General
The risk of infection of staff is very low and is only before the patient has been treated with suitable antibiotics for 24 hours or more (parenteral ceftriaxone or benzyl penicillin). In one study the absolute risk to healthcare workers was estimated as less than 1 in 100,000[1]. There is no evidence of increased risk from medical or nursing care that does not involve direct contact with respiratory secretions or droplets. The greatest risk to staff is during intubation or other airway management procedures that produce large droplet aerosols while not wearing a mask. Exposure by a patient coughing onto the health care worker’s face may also increase risk [1-3].
1.1.1. There is no evidence that there is any increased risk to the family or other contacts of staff.
1.2. Primary Prevention
The risk of infection for healthcare workers is controlled by:
a) Treatment of the patient – standard treatment with ceftriaxone should eradicate carriage within 24 hours.
b) Using personal protective equipment, in particular a correctly fitted FFP3 mask, when intubating or suctioning a patient or having other contact likely to produce direct contact with respiratory secretions. Direct contact with patient respiratory secretions such as intubation, aerosols produced at suctioning or face-to-face contact is the most important risk factor.
1.3. Secondary prevention
1.3.1. Antibiotic chemoprophylaxis is recommended if a staff member is exposed to a probable or confirmed patient’s respiratory secretions during acute illness before completing 24 hours of systemic antibiotics. This includes either a history of contact between respiratory secretions and the staff member’s face or a history of performing an at-risk procedure, such as intubation, without protection. (NB: a lumbar puncture is not considered an at-risk procedure.)
1.3.2. Antibiotic chemoprophylaxis eradicates carriage of the infection and may protect this person against disease. It also protects against spread of infection from the person who takes the chemoprophylaxis, although there is no evidence for disease arising in contacts of healthcare workers with or without chemoprophylaxis.
1.3.3. Chemoprophylaxis is not needed for those involved in other forms of healthcare or for those wearing FFP3 masks. Widespread use of chemoprophylaxis is associated with adverse events and the risk from unwarranted treatment is unacceptable given the lack of hazard except for those with an unprotected exposure. [1]
1.3.4. If staff have been exposed contact OUHFT Centre for Occupational Health and Wellbeing (COHWB) during normal working hours or OUHFT Microbiology out of hours via switchboard for a risk assessment. OUHFT will risk assess staff with help, if required, from the health protection team (UKHSA) and decide who requires antibiotic prophylaxis.
1.3.5. If antibiotic prophylaxis is required in-hours then it will be supplied by Occupational health using a Patient Group Direction (PGD). Occupational health will liaise directly with the staff member and/ or GP if the staff member is unable to attend the COHWB to ensure the timely supply of prophylaxis.
1.3.6. If antibiotic prophylaxis is required out-of-hours then the staff member can either:
- attend ED out of hours where the team will review and prescribe the prophylaxis, or,
- attend COHWB at a convenient time (see note 1.3.7 below).
1.3.7. Chemoprophylaxis should be administered as soon as possible ideally within 24 hours but can be administered up to four weeks after exposure.
2. Patient’s relatives or close contacts
2.1. Health protection staff (UKHSA) will risk assess the relatives and close contacts of a patient with (probable or confirmed) meningococcal infection. They will also provide advice on antibiotics. OUHFT will only supply chemoprophylaxis for household equivalent contacts identified by UKHSA where it is felt to be inappropriate to send the contact to obtain chemoprophylaxis in the community (e.g. parents or partner of critically ill patient who wish to remain at their bedside).
2.2. Bedside relatives requiring antibiotic prophylaxis should be reviewed by the ED team (adults or paediatrics) who will prescribe the antibiotics. Ciprofloxacin will be administered within the ED department. Rifampicin will need to be prescribed on a discharge prescription and be supplied via pharmacy.
2.2.1 Chemoprophylaxis is not an emergency, and Rifampicin will not be supplied by OUHFT Pharmacy overnight. The prescription can wait until pharmacy staff are on site the following morning (i.e. after 8am).
3. Recommended chemoprophylaxis for those with significant risk of infection
Ciprofloxacin is the recommended choice for meningococcal chemoprophylaxis. However there have been increasing reports of ciprofloxacin resistance among invasive meningococcal strains in the Middle East and Asia therefore Rifampicin is recommended for first-line prophylaxis in close contact of cases with recent travel to the Middle East or Asia.
Patients receiving ciprofloxacin must be counselled about possible side effects of fluoroquinolones. Use the MHRA patient information leaflet to support discussions, available HERE
| Drug | Dose, frequency & duration | Quantity supplied | |
| Adults (1st choice) | ciprofloxacin | 500mg oral single dose | 1x 500mg tablet |
| Adults (alternative or 1st line in close contact with case with recent travel to Middle East or Asia) | rifampicin | 600mg oral BD for 2 days | 8x 300mg capsules |
| Pregnant women | ciprofloxacin | 500mg oral single dose | 1x 500mg tablet |
| Children: | (see below for age and weight appropriate doses) | ||
|
Children (1st choice) Age 0 months to 18 years |
ciprofloxacin |
dose: see table below oral single dose |
1x 250mg or 500mg tablet (tablets can be halved and disperses easily in water) |
|
Children (alternative or 1st line in close contact with case with recent travel to Middle East or Asia) Age 0 months to 18 years |
rifampicin |
dose: see table below oral BD for 2 days |
supply 100mg/5ml oral liquid |
Doses for children
Oral ciprofloxacin
| Age |
Dose of oral ciprofloxacin |
|
Under 1 year |
30 mg/kg (max 125 mg) po single dose |
|
1 year to 4 years |
125 mg po single dose |
|
5 years to 11 years |
250 mg po single dose |
|
12 years to 18 years |
500 mg po single dose |
Doses are as per UKHSA (2024) Guidance for public health management of meningococcal disease in the UK (page 28)
Patients receiving ciprofloxacin must be counselled about possible side effects of fluoroquinolones. Use the MHRA patient information leaflet to support discussions, available HERE
Oral rifampicin
| Age |
Dose of oral rifampicin |
|
Under 1 year |
5 mg/kg po BD for 2 days |
|
1 year to 11 years |
10 mg/kg (max 600 mg per dose) po BD for 2 days |
|
12 years to 18 years |
600 mg po BD for 2 days |
Summary
- The Health Protection Team (UKHSA) will risk assess patient contacts and advise on prescription.
- OUHFT staff will risk assess staff contacts seeking advice from the Health Protection Team (UKHSA) as required.
- OUHFT will inform COHWB regarding any healthcare workers needing prophylaxis in hours and will contact Microbiology out of hours.
- If antibiotic prophylaxis is required in-hours then it will be supplied by COHWB using a PGD.
- If antibiotic prophylaxis is required out-of-hours then the staff member can:
- attend ED out of hours where the team will review and prescribe the prophylaxis, or,
- attend COHWB at a convenient time. Chemoprophylaxis should be administered as soon as possible ideally within 24 hours but can be administered up to four weeks after exposure.
References
- UK Health Security Agency. Guidance for public health management of meningococcal disease in the UK. 2024.
- Riccò M, Vezzosi L, Odone A, Signorelli C. Invasive meningococcal disease on the workplaces: a systematic review. Acta Bio Medica Atenei Parm. 2017;88(3):337.
- Gilmore A, Stuart J, Andrews N. Risk of secondary meningococcal disease in health-care workers. The Lancet. 2000 Nov 11;356(9242):1654–5.