Pain Despite Epidural
Basic Approach
Points to Consider
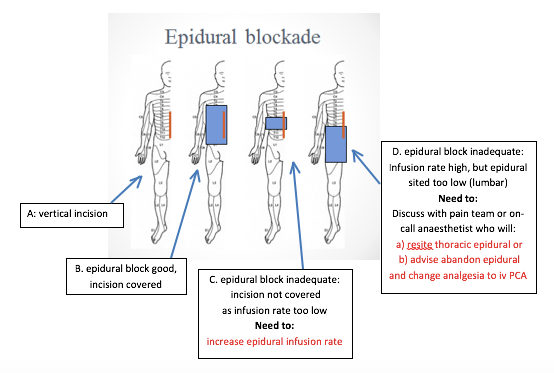
1. If a patient describes pain while receiving epidural analgesia, it may be that the infusion rate is insufficient to cover the pain distribution. By increasing the epidural infusion rate, the spread (or height) of the block is increased, so a higher infusion rate (up to a maximum of 12ml/hr) may be all that’s needed. [This is also the reason why it makes no sense to “wean” an effective epidural.]
2. The epidural catheter may have become dislodged or disconnected, so it is wise to check the patient’s back to ensure that the dressing over the epidural insertion site is intact and the catheter still in place.
3. Occasionally an epidural may provide a unilateral block. The pain team or on-call anaesthetist may be able to adjust the catheter to give a more balanced block.
4. Despite the maximum infusion rate and an apparently well-placed catheter, some epidurals do not provide sufficient analgesia. The pain team or on-call anaesthetist may be able to give an epidural bolus dose to re-establish a block or arrange for a resite (See Useful Contact Details within OUH) .
5. If, for whatever reason, epidural analgesia is not effective, the pain team or on-call anaesthetist should be called. If the patient is in pain and there is likely to be a delay in getting specialist advice:
- Stop the epidural infusion but leave the catheter in place and connected to the pump
- Start alternative analgesia, eg iv PCA ( Starting a PCA)
- As the epidural infusate contains an opioid (fentanyl) the PCA should be bolus only, with no background, to avoid opioid accumulation.